Selective Neck Dissection in N0 Papillary Thyroid Carcinoma
Abstract
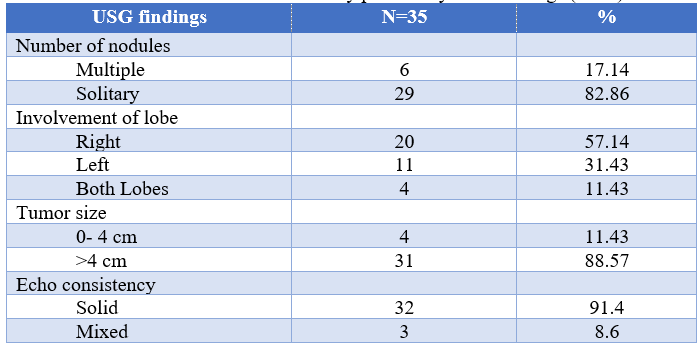
Background: Papillary thyroid carcinoma is the most common form of well differentiated thyroid cancer and constitutes 1% of all solid tissue cancers with a female predominance. Surgical intervention helps in removal of lesion. Lymph node metastasis in cervical compartments is the main reason of recurrence of disease. Personalized risk stratified prophylactic neck dissection at initial thyroidectomy in Papillary thyroid carcinoma with no clinical, sonographic or per-operative evidence of lymph node metastasis has been advocated, though not unanimously. Compartment oriented lymph node dissection in patients with PTC reduces recurrence and improves survival. Objectives: The aim of this study is to determine the Role of selective neck dissection in case of N0 papillary thyroid carcinoma. Methods: A cross-sectional prospective study was conducted in the Dept of Otolaryngology and Head neck surgery, BSMMU, Dhaka for one and a half years from September/2021 to February/2023, with 35 patients underwent total thyroidectomy with selective neck dissection (level VI, III, IV, II) for N0 Papillary thyroid carcinoma. All patients were evaluated by complete clinical head & neck examination, thyroid hormone profile, ultrasonography finding, fine needle aspiration cytology, radiology and histopathology report were recorded. Data were analyzed statistically by using by Statistical Package for Social Scientist (SPSS-24). Results: The age was ranged from 22 to 70 years with mean age was 47.77±14.8 years. Male to female ratio was 1:2.2. 17.4% patients had multiple number of nodules and 82.86% patients had solitary nodule. 11.43 % patients had involvement of both lobes, 31.43 % had involvement of left lobe, 57.14% had involvement of right lobe. More than three-fourth (88.57%) patients, tumor size >4 cm and in case of 11.43% patients, tumor size is within 0- 4 cm. 8.6% patients had mixed echo consistency and 91.4% had solid echo consistency. Conclusion: Most of the patients were in 6th and above decade and female predominant. Solitary nodule, right lobe involvement, size more than 4cm and solid echo consistency were more frequent. Regarding selective neck dissection; 17.1% had metastasis at level VI and no metastasis at level II, III, IV. In brief, 17.1% patients had metastasis on histopathology after neck dissection and 82.9% patients had no metastasis on histopathology after neck dissection. It can be said that, Central compartment neck dissection has role in detecting metastasis at N0 stage of Papillary thyroid carcinoma but Lateral neck dissection has no role in detecting metastasis at N0 stage of Papillary thyroid carcinoma.
Downloads
References
Siegel RL, Miller KD, Jemal A. Cancer statistics, 2019. CA: a cancer journal for clinicians. 2019 Jan;69(1):7-34.
Chen W, Li J, Peng S, Hong S, Xu H, Lin B, Liang X, Liu Y, Liang J, Zhang Z, Ye Y. Association of total thyroidectomy or thyroid lobectomy with the quality of life in patients with differentiated thyroid cancer with low to intermediate risk of recurrence. JAMA surgery. 2022 Mar 1;157(3):200-9.
Nickel B, Tan T, Cvejic E, Baade P, McLeod DS, Pandeya N, Youl P, McCaffery K, Jordan S. Health-related quality of life after diagnosis and treatment of differentiated thyroid cancer and association with type of surgical treatment. JAMA otolaryngology–head & neck surgery. 2019 Mar 1;145(3):231-8.
Moorthy R, Kumar S, Warfield AT. Thyroid and parathyroid gland pathology. InScott-Brown's Otorhinolaryngology and Head and Neck Surgery 2018 Jun 12 (pp. 651-703). CRC Press.
Aoyama M, Inui T, Miyamoto N, Sakamoto S, Inoue S, Fujiwara S, Goto M, Toba H, Takizawa H. A case of papillary thyroid carcinoma with renal and pulmonary metastases. Journal of Surgical Case Reports. 2022 Aug;2022(8): rjac366.
Liu Y, Wang Y, Zhao K, Li D, Chen Z, Jiang R, Wang X, He X. Lymph node metastasis in young and middle-aged papillary thyroid carcinoma patients: a SEER-based cohort study. BMC cancer. 2020 Dec; 20:1-2.
Yang J, Zhang F, Qiao Y. Diagnostic accuracy of ultrasound, CT and their combination in detecting cervical lymph node metastasis in patients with papillary thyroid cancer: a systematic review and meta-analysis. BMJ open. 2022 Jul 1;12(7): e051568.
Neiderman NN, Baris H, Duek I, Warshavsky A, Ringel B, Izkhakov E, Horowitz G, Fliss DM. Lateral neck dissection for well-differentiated thyroid carcinoma: is prophylactic level V neck dissection necessary? A retrospective cohort study. Ear, Nose & Throat Journal. 2023 Jul;102(7):NP349-57.
Medas F, Canu GL, Cappellacci F, Anedda G, Conzo G, Erdas E, Calò PG. Prophylactic central lymph node dissection improves disease-free survival in patients with intermediate and high risk differentiated thyroid carcinoma: a retrospective analysis on 399 patients. Cancers. 2020 Jun 23;12(6):1658.
Altiner S, Kozan R, Emral AC, Taneri F, Karamercan A. Effects of patient and tumor characteristics on central lymph node metastasis in papillary thyroid cancer: a guide for selective node dissection. Archives of Iranian medicine. 2022 Nov;25(11):730.
Kadhim SH, Mahmood KI, Habash MM. The Role of Prophylactic Cervical Lymph Node Dissection with Total Thyroidectomy in Prevention Recurrence of Papillary Thyroid Carcinoma. Open Access Macedonian Journal of Medical Sciences. 2022 May 10;10(B):1372-6.
Ducoudray R, Trésallet C, Godiris-Petit G, Tissier F, Leenhardt L, Menegaux F. Prophylactic lymph node dissection in papillary thyroid carcinoma: is there a place for lateral neck dissection? World journal of surgery. 2013 Jul; 37:1584-91.
Eltelety AM, Terris DJ. Neck dissection in the surgical treatment of thyroid cancer. Endocrinology and Metabolism Clinics. 2019 Mar 1;48(1):143-51.
Suresh GM, Halkud R, Arjunan R, Ramachandra C, Altaf S, Pandey D, Krishnamurthy S. Amalgamation of Central Lymph Node Dissection in Papillary Thyroid Carcinoma: Study from South Indian Population. Indian Journal of Otolaryngology and Head & Neck Surgery. 2019 Oct; 71:939-43.
Chowdhury SR, Khan Y, Kamal A, Kamal AH, Talukder MH. Evaluation of the Outcome of Patients with Papillary Thyroid Carcinoma with Surgical Intervention. Chattagram Maa-O-Shishu Hospital Medical College Journal. 2016;15(2):52-6.
Kadhim SH, Mahmood KI, Habash MM. The Role of Prophylactic Cervical Lymph Node Dissection with Total Thyroidectomy in Prevention Recurrence of Papillary Thyroid Carcinoma. Open Access Macedonian Journal of Medical Sciences. 2022 May 10;10(B):1372-6.