Serum magnesium level in patients with acute myocardial infarction and its relation with arrhythmia
Abstract
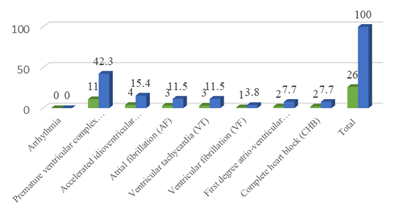
Introduction: Magnesium (Mg) is the second most common intracellular cation after potassium (K). Mg is a cofactor in many enzyme systems in human cells and it has a predominant role in normal myocardial physiology. The role of magnesium in cardiovascular disease has received widespread attention. Magnesium has been implicated in the complications like arrhythmias in acute myocardial infarction. Objective: To know the serum magnesium level in patients with acute myocardial infarction and its relation with arrhythmia. Methods: A descriptive cross-sectional study was conducted in the Department of Cardiology, Sheikh Fazilatunnessa Mujib Memorial KPJ Specialized Hospital, Gazipur, Bangladesh from January 2020 to June 2020. 50 patients with acute myocardial infarction were admitted. Data were collected from patients of any age and both sexes with acute myocardial infarction as determined by clinical features, ECG evidence and biochemical report. A blood sample for estimation of serum magnesium level was collected as early as possible within 24 hours of admission and the 5th day of admission. After admission to CCU, every patient was under continuous cardiac monitoring to see and record any arrhythmia within 5 days’ onset of symptoms. Results: A total of 50 patients with acute myocardial infarction were included during the study period. The male to female ratio in the study group was 3.17:1 and the maximum incidence of acute myocardial infarction was seen in the 5th and 6th decade. The most common presenting symptom was chest pain which was present in all patients and was associated with sweat in 60% of patients and breathlessness in 64% of patients and palpitation in 50%. In the study, the most common risk factor found was smoking (70%) followed by diabetes (36%) and hypertension (30%). Anterior wall MI was found to be the most common type of MI (42%). Arrhythmia developed in (52%) patients and in the majority (57.7%) with anterior wall MI. In the study group mean serum magnesium level in 50 patients on day-1 is 1.86±0.39 and on Day-5 is 2.26±0.5. The mean serum magnesium level in 26 patients with arrhythmia was 1.65±0.26 on day-1 and 1.98±0.25 on day-5. In the study group, the mean serum magnesium level in 24 patients without arrhythmia was 2.05±0.41 on day-1 and 2.48±0.52 on day-5. The difference between the magnesium level in patients with arrhythmia and without arrhythmia is statically significant on both days- 1 and day-5 (p<0.001). PVC was the most common type (42.5%) of arrhythmia. Conclusion: serum magnesium levels are significantly low in patients who develop arrhythmia in acute myocardial infarction.
Downloads
References
Lopez AD, Murray CC. The global burden of ischemic heart disease 1990-2020. Nat Med 1998; 4:1241-1249.
Khondokar RK, Hossain D, Hossain M. Retrospective analysis of acute myocardial infarction. Bang Heart J 1987; 1:14.
Islam MN, Ali MA & Ali M. ‘Spectrum of cardiovascular disease: the current scenario in Bangladesh’, Bangladesh Heart J, 2004; 19:1-7.
Richard W Bunton. Value of serum magnesium estimation in diagnosing myocardial infarction and predicting dysrhythmias after coronary artery bypass grafting Thorax 1983; 38:946-950
Jeremias A, Bertschat FL, Jeremias E, Ising H. Possible Correlation between Decrease of Ionized Magnesium. and Calcium in Blood to Patient Outcome after Acute Myocardial Infarction J Clin Basic Cardiol 2000; 3: 124
Wecker Wec, Parisi AF. Magnesium metabolism. N Engl J Med. 1968; 278: 658-663
Ebel H, Günther T. Role of Magnesium in Cardiac Disease J. Clin. Chem. Clin. Bipchem 1983; 21: 249-265
Whang R, Chrysant S, Dillard B. Hypomagnesemia and hypokalaemia in 1000 treated ambulatory hypertensive patients. J Am Coll Nutr. 1982; 1: 317.
Elliott M. Antman Magnesium in Acute MI Circulation. 1995; 92(9): 2367-2372.
Woods Kl, Florcurs R, Haider Y. Intravenous magnesium sulphate injections in suspected acute myocardial infarction patients effects of the second Leircaster intravenous magnesium international trial (LIMIT- II) Lancet 1992; 339: 1553-1558.
Ahmed A, Junjua BA, Rizvi SFUH, Tanveer ZH, Ahmed I. Prevalence of hypomagnesaemia in patients with acute Myocardial infarction compared with normal subjects. Sheikh Zayed Medical College J 2010; 4: 6-8.
Ahmad A, Tanvir ZH, Hussain Z. Acute myocardial infarction; Serum magnesium and electrolyte levels at presentation in emergency department. Professional Med J 2010; 17(2): 246-251.
Autman EM, Magnesium in acute myocardial infarction: Overview of the available evidence. Am heart J. 1996: 132: 487-494.
Abraham A, Shaoul R, Shimonovitz S. Serum magnesium levels in Acute Medical and Surgical Conditions. Biochemical Medicine 1980; 24: 21
Babel S, Bhatnagar HNS, Bhatnagar BK. Serum magnesium levels in cases of acute myocardial infarction and its prognostic significance. JAPI. 1983; 31: 755-7.
Choudhury MBK, Rahman MS, Hassan MM, Begum R, Hoque N, Akhtaruzzaman M, Chowdhury AN. Comparison of Serum Magnesium and Potassium in Acute Myocardial Infarction and Chronic Ischemic Heart Disease J. Dhaka National Med. Coll. Hos. 2011; 17 (01): 33-36
Haigney MCP, Silver B, Tanglao E, Silverman HS, Hill D, Shapiro E, Gerstenblith G, Schulman SP. Intracellular magnesium levels in acute myocardial infarction. Circulation. 1995; 92.
Gupta R, Joshi P, V Mohan V, et al. Epidemiology and causation of coronary heart disease and stroke in India. Heart 2008; 94:16-26.
French JK, White HD. Clinical implications of the new definition of myocardial infarction. Heart 2004; 90:99-106.
Dyckner T. Serum magnesium in acute myocardial infarction: Relation to Arrhythmias. Acta med scan 1980, 207:59-66.
Steg PG, Goldberg RJ, Gore JM, Fox KAA et al. Baseline Characteristics, Management Practices, and In-Hospital Outcomes of Patients Hospitalized with Acute Coronary Syndromes in the Global Registry of Acute Coronary Events (GRACE). The American Journal of cardiology 2002:90:358-363.
Kelly AM, Klim S. How common are ventricular arrhythmias in patients admitted to CCU with chest pain and a non-eschemic ECG? A pilot study. Heart Asia 2011:48-50.
Yadav P, Joseph D, Joshi P, Sakhi P, Jha RK, Gupta J. Clinical profile & risk factors in acute coronary syndrome. National Journal of community Medicine 2010:1:2:150-2.
Misiriya KJR, Sudhayakumar N, Khadar SA, George R, Jayaprakash VL, Pappachan JM. The Clinical Spectrum of Acute Coronary Syndromes: Experience from a Major Center in Kerala: Association of Physicians of India 2009.
Abraham A, Shaoul R, Shimonovitz S et al. Serum magnesium levels in Acute Medical and Surgical Conditions. Biochemical Medicine. 1980; 24: 21.
Sachadeva et al. Serum magnesium and platelet adhesiveness in acute myocardial infarction. JIMA. 1978; 71: 165.
Dyckner T. Serum magnesium in acute myocardial infarction: Relation to Arrhythmias. Acta med scan 1980, 207:59-66.