Effect of dyslipidemia and its association with coronary artery disease on angiographic findings
Abstract
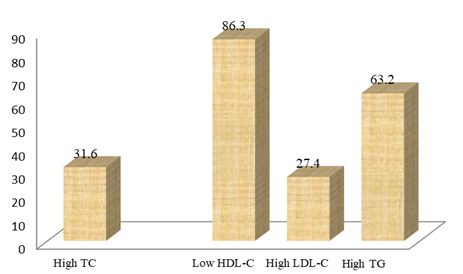
Introduction: Dyslipidemia is an abnormal amount of lipids in the blood which act as a most common risk factor for CAD. In developed countries, most dyslipidemias are hyperlipidemias; that is, an elevation of lipids in the blood. This is often due to diet and lifestyle. Prolonged elevation of insulin levels can also lead to dyslipidemia. Objective: To assess the effect of dyslipidemia and its association with coronary artery disease on angiographic findings. Methods: This was a retrospective cross-sectional study was carried out at Cardiology Department, Bangladesh Medical College Hospital, Dhaka, Bangladesh from January to December 2021. Information was gathered from medical records of patients admitted for coronary angiography in our Hospital. During the study period 112 consecutive patients, suffering from CAD were examined. Coronary angiography was performed in the catheterization laboratory of the institute and interpreted by interventionist cardiologists. Reporting was done regarding the stenosis percentage of the main epicardial coronary arteries, and the extent of CAD was categorized as one-vessel, two-vessel, or three-vessel disease, according to the number of affected vessels. Statistical analysis was performed with SPSS version 20 (SPSS, Inc., Chicago, IL, USA) statistical software. Results: During the study period, we identified 112 patients who were subjected to coronary angiography. The mean age of patients were 54.40 years (±SD 8.78 years), where the minimum age was 28 and maximum age was 75. Majority of the patients were young, with around 40.1% (45) of the patients age 46-55 years. The study consisted predominantly of males as represented by 84.82% of the patients, while 15.17% were females. The lipid profile analysis revealed that the mean total cholesterol was 182.60 ± 54.41 mg/dl, mean low-density lipoprotein cholesterol (LDL-C) was 105.46 ± 40.85 mg/dl, mean high density lipoprotein cholesterol (HDL-C) was low, 34.26 ± 7.234 mg/dl and mean triglyceride level was high, 207.64 ± 151.20 mg/dl. The mean levels of different lipids. the patients where dyslipidemia were present in 75.89% patients. Distribution of types of myocardial infarction among the patients. Among 112 patients there were patients of inferior MI 33%, anterior MI 22%, extensive anterior MI 10%, anteroseptal MI 18.5%, Inferolateral MI 9%, lateral MI 4%, high lateral MI 2% and anteroinferior 1.5%. In patients according to clinical findings where mean ± SD of systolic blood pressure was found 134.75 ± 19.25 and random blood sugar was found in 223.81 ± 72.18 mg/dl as well as gallop rhythm was found in 11% patients, those are remarkable. In this study, the most frequent form of dyslipidemia among the patients with significant CAD was found to be low levels of HDL-C (<40mg/dL) at 86.3%, followed by high TG levels (≥150mg/dL) to be 63.2%, high levels of total cholesterol (≥200mg/dl) at 31.6%, and high LDL-C (≥130mg/dL) to be 27.4%. In hospital stay of the patients where mean ± SD of hospital stay of the study patients was 6±0.88 days. 57.1% patients got improved with better outcome and discharged after treatment.
Downloads
References
Berger CJ, Murabito JM, Evam JC. Prognosis after first myocardial infarction: comparison of Q-wave and Non Q-wave myocardial infarction in the framingham–heart study. JAMA 1992; 268: 1545-46.
Cooper H, Panza JA. Q wave to guide treatment of myocardial infarction.Lancet 2006 24(367):2035-2037.
Antman EM, Braunwald E.ST-elevation myocardial infarction. In: Libby P,Bonow RO, Mann DL, Zipes DP. Eds. Braunwald’s heart disease. 8th ed. Philadelphia, USA: Saunders; 2008. 1221-1222
Washio M, Sasazuki S, Kodama H et al. Role of hypertension, dyslipidemia and diabetes mellitus in the development of coronary atherosclerosis in Japan. Jpn Circ J. 2001;65:731-7.
Haastrup B, Rohold A, Larsen S et al. Prevalence of dyslipidemia in patients admitted for coronary angiography. Atherosclerosis. 1995;115:34-34(1).
Khanal S, Obeidat O, Lu M, et al. Dyslipidemia in patients with angiographically confirmed coronary artery disease. An opportunity for improvement. Clin Cardiol. 2004;27:577-80.
Phababpha S, Intharaphet P, Duangsorn S, et al. Association of dyslipidemia with coronary artery stenosis in coronary artery disease patients. Thai J Pharmacol. 2009;31:107-10.
Bittner V. Perspectives on dyslipidemia and coronary heart disease in women. J Am Coll Cardiol. 2005;46:1628-35.
Hokanson J, Austin M. Plasma triglyceride level is a risk factor for cardiovascular disease independent of high-density lipoprotein cholesterol level: a meta-analysis of populationbased prospective studies. J Cardiovasc Risk. 2009;3:213-9.
González-Pacheco H, Vargas-Barrón J, Vallejo M, Piña-Reyna Y, Altamirano-Castillo A, Sánchez-Tapia P, Martínez-Sánchez C. Prevalence of conventional risk factors and lipid profiles in patients with acute coronary syndrome and significant coronary disease. Therapeutics and clinical risk management. 2014;10:815.
Grundy SM, Pasternak R, Greenland P, Smith S, Fuster V. Assessment of cardiovascular risk by use of multiple-risk-factor assessment equations: a statement for healthcare professionals from the American Heart Association and the American College of Cardiology. Circulation. 1999;100(13):1481–1492.
Pasternak RC, Grundy SM, Levy D, Thompson PD. 27th Bethesda Conference: matching the intensity of risk factor management with the hazard for coronary disease events. Task Force 3. Spectrum of risk factors for coronary heart disease. J Am Coll Cardiol. 1996;27(5):978–990.
Torremocha F, Hadjadj S, Carrie F, et al. Prediction of major coronary events by coronary risk profile and silent myocardial ischemia: prospective follow up study of primary prevention in 72 diabetic patients. Diabetes Metab. 2001;27:49-57.
Kosaka S, Okuda F, Satoh A, et al. Effect of coronary risk factors on coronary angiographic morphology in patients with ischemic heart disease. Jpn Circ J. 1997;61:390-5.
Bashore TM , Granger CB, Hranitzky P , Patel MR. Coronary heart disease. In: McPhee S,Papakadias MA. Eds. Current medical diagnosis and treatment. 49thed. New York, USA: McGraw Hill; 2010; 317.
Alam, Md Zahid, Aparna Rahman, Shabnam Jahan Hoque, SM RezaulIrfan, Md Babul Miah, and Mohammad ShakhawatHossain. "Pattern of Dyslipidemia in different type of Myocardial Infarction." Bangladesh Critical Care Jmynal 5, no. 2: 106-109.
Murray CJL, Lopez AD. The global burden of disease: a comprehensive assessment of mortality and disability from disease, injuries and risk factors in 1990 and projected to 2020. Harvard School of Health, Boston (Mass) (1996)
Maron DJ. The epidemiology of low levels of high-density lipoprotein cholesterol in patients with and without coronary artery disease. The American journal of cardiology. 2000 Dec 21;86(12):11-4
Gupta R, Gupta VP, Sarna M, Bhatnagar S, Thanvi J, Sharma V, Singh AK, Gupta JB, Kaul V. Prevalence of coronary heart disease and risk factors in an urban Indian population: Jaipur Heart Watch-2. Indian heart journal. 2002;54(1):59-66.
Goel PK, Bharti BB, Pandey CM, et al. A tertiary care hospital-based study of conventional risk factors including lipid profile in proven coronary artery disease. Indian Heart J. 2003;55:234–40.
Mohan V, Deepa R, Rani SS, et al. Prevalence of coronary artery disease and its relationship to lipid in a selected population in South India. J Am Coll Cardiol. 2001;38:682–7.
The European Atherosclerosis Society Consensus Panel. Triglyceride-rich lipoprotein and high-density lipoprotein cholesterol in patients at high risk of cardiovascular disease: evidence and guidance for management. Eur Heart J 2011
Reddy KS, Prabhakaran D, Chaturvedi V, Jeemon P, Thankappan KR, Ramakrishnan L et al.; Methods forestablishing a surveillance system for cardiovascular diseases in Indian industrial populations. Bulletin of the World Health Organization, 2006; 84: 461-467
Peter B, Richman MD. Clinical characteristics of Diabetic vs Nondiabetic Patients Who ”Rule in” for Acute Myocardial Infarction. Academic Emergency Medicine 1999;6(7):719-23.
Boucher JM. On behalf of the Quebec Acute Coronary Care Working Group Age- related differences in in-hospital mortality and the use of thrombolytic therapy for acute myocardial infarction. CMAJ 2001;164(9):1285-90
Culie V. Acute myocardial infarction: Differing preinfraction and clinical features according to infarct site and gender. Int J Cardiol 2003; 90(2-3):189-96.
Shepherd J, Hunnihake D, Barter P, et al. Guidelines for lowering lipids to reduce coronary artery disease risk: A comparison of rosuvastatin with atorvastatin, pravastatin, and simvastatin for achieving lipid-lowering goals. Am J Cardiol. 2003;91:11-7.