Progression of left ventricular ejection fraction after acute myocardial infarction
Abstract
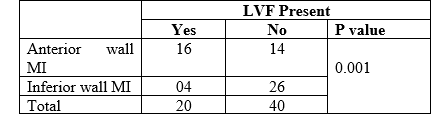
Introduction: A significant proportion of deaths in patients with chronic ischemic cardiomyopathy are due to heart failure or sudden cardiac death (SCD) [1]. Numerous clinical trials have confirmed the benefit of implantable cardioverter-defibrillator (ICD) treatment in patients with reduced left ventricular (LV) function after an acute myocardial infarction (AMI). Objective: To measure and compare Left Ventricular Ejection Fraction (LVEF) after acute anterior wall and inferior wall myocardial Infarction and correlate LVEF with clinical findings in the patients. Methods: It was a prospective observational echocardiography based study which was carried out in the Dept. of Cardiology, Shaheed Tajuddin Ahmad Medical College Hospital, Gazipur, Bangladesh from March to October 2022. A total of 60 (sixty) patients of (anterior or inferior) Acute Myocardial infarction (AMI) were included in the study. Patients were divided in two groups on the basis of anterior myocardial wall MI (AWMI) or inferior myocardial wall MI (IWMI). Echocardiography was done on all cases and ejection fraction was calculated by applying Simpson’s Rule and patients were examined at the same time to see the presence of signs of left ventricular failure (LVF). (LVEF) was correlated with the findings of LVF in these patients. Results: Out of 30 patients of anterior wall MI, 18 (60%) were male and 12 (40%) were female. In inferior wall MI, 28 (93.3%) were male and 2 (6.7%) were female. In all 60 patients (76.7%) patients were male and (23.3%) were females. In anterior wall MI, (6.7%) were in 30 to 40 years of age, (33.3%) were in 41 to 50 years of age, (33.3) were in 51 to 60 years of age, (20.0%) were in 61 to 70 years of age, and (6.7%) were in 71 to 80 years of age. Minimum age was 39 years; maximum was 72 years, with mean of 54.57 and SD of 9.22. In patients with LVF mean ejection fraction (EF) was 37.13 with standard deviation (SD) of 8.4 %. In patients without failure the mean EF was 56.29% with SD of 3.75. In 30 patients of IWMI, mean EF was 54.93% with SD of 6.86. In 30 patients of AWMI it was 46.07% with SD of 11.72. In all 60 patients minimum EF was 30% and maximum was 60% with a mean of 50.50 with SD of 10.52. In AWMI, 53% patients had signs of left ventricular failure. In patients of IWMI, 13.3% had signs of LVF. Conclusions: AWMI causes more decrease in LVEF. LVF is more commonly associated with AWMI than IWMI. There is statistically significant difference in LVEF of patients with and without LVF.
Downloads
References
Moss AJ, Hall WJ, Cannom DS, Daubert JP, Higgins SL, Klein H, Levine JH, Saksena S, Waldo AL, Wilber D, Brown MW, Heo M. Improved survival with an implanted defibrillator in patients with coronary disease at high risk for ventricular arrhythmia: Multicenter Automatic Defibrillator Implantation Trial Investigators.N Engl J Med. 1996; 335:1933–1940.
Buxton AE, Lee KL, Fisher JD, Josephson ME, Prystowsky EN, Hafley G. A randomized study of the prevention of sudden death in patients with coronary artery disease: Multicenter Unsustained Tachycardia Trial Investigators.N Engl J Med. 1999; 341:1882–1890.
Antman EM, Braunwald E. Acute myocardial infarction. In: Braunwald E, Fauci AS, Isselbacher KJ, Wilson JD, Martin JB, Kasper DL et al eds. Harrison’s Principles of internal medicine .New York:McGraw-Hill, 1998: 1352-65.
Awan ZA, Mufti W. First year mortality and morbidity after AMI in Peshawar. J Ayub Med Coll 1996; 8: 3-5.
Haq I. In-hospital mortality after acute myocardial infarction. Specialist, 1993; 9: 249-51
Greenberg H, Case RB, Moss AJ, Brown MW, Carroll ER, Andrews ML; MADIT-II Investigators. Analysis of mortality events in the Multicenter Automatic Defibrillator Implantation Trial (MADIT-II).J Am Coll Cardiol. 2004; 43:1459–1465.
Steinbeck G, Andresen D, Seidl K, Brachmann J, Hoffmann E, Wojciechowski D, Kornacewicz-Jach Z, Sredniawa B, Lupkovics G, Hofgärtner F, Lubinski A, Rosenqvist M, Habets A, Wegscheider K, Senges J; IRIS Investigators. Defibrillator implantation early after myocardial infarction.N Engl J Med. 2009; 361:1427–1436.
Adabag AS, Therneau TM, Gersh BJ, Weston SA, Roger VL. Sudden death after myocardial infarction. JAMA. 2008; 300:2022–2029.
Solomon SD, Zelenkofske S, McMurray JJ, Finn PV, Velazquez E, Ertl G, Harsanyi A, Rouleau JL, Maggioni A, Kober L, White H, Van de Werf F, Pieper K, Califf RM, Pfeffer MA; Valsartan in Acute Myocardial Infarction Trial (VALIANT) Investigators. Sudden death in patients with myocardial infarction and left ventricular dysfunction, heart failure, or both.N Engl J Med. 2005; 352:2581–2588.
Hohnloser SH, Kuck KH, Dorian P, Roberts RS, Hampton JR, Hatala R, Fain E, Gent M, Connolly SJ; DINAMIT Investigators. Prophylactic use of an implantable cardioverter-defibrillator after acute myocardial infarction.N Engl J Med. 2004; 351:2481–2488.
Dorian P, Hohnloser SH, Thorpe KE, Roberts RS, Kuck KH, Gent M, Connolly SJ. Mechanisms underlying the lack of effect of implantable cardioverter-defibrillator therapy on mortality in high-risk patients with recent myocardial infarction: insights from the Defibrillation in Acute Myocardial Infarction Trial (DINAMIT).Circulation. 2010; 122:2645–2652.
Braunwald E, Rutherford JD. Reversible ischemic left ventricular dysfunction: evidence for the “hibernating myocardium.”J Am Coll Cardiol. 1986; 8:1467–1470.
Karim MA, Mehmood SF, Akhtar J, Qureshi J. Thrombolytic therapy in AMI in Pakistan. J Pak Med Assoc. 1995; 45: 54-8.
Kyne L, Hausdorff JM, Knight E, Dukas L, Azhar G, Wei JY. Neutrophilia and congestive heart failure after acute myocardial infarction. Am Heart J. 2000; 139: 94- 100.
Sola M, Margrina J, Pavia J, Vidal-Sicart S, Huguet M, Pare C, et al. Predictive value of 99 Tcm-Sestamibi gated SPECT for long-term myocardial perfusion and recovery after acute myocardial infarction. Nucl Med Commun 1998; 19: 823-30.
Senior R, Basu S, Kinsey C, Schaeffer S, Lahiri A. Carvedilol prevents remodeling in patients with left ventricular dysfunction after acute myocardial infarction. Am Heart J 1999; 137 (4 pt.1): 646–52.
Ali AS, Rybicki BA, Alam M, Wulbercht N, Kicher-CornishK, Khaja F, et- al. Clinical predictors of heart failure in patients with first acute myocardial infarction. Am Heart J 1999; 138: 1133-9.
Vaur L, Danchin N, Genes N, Renault M,etienne S, Ferriers, et al. Characteristics of patients hospitalized for myocardial infarction in France with respect to left ventricular dysfunction. Arch Mal Coer–Vaiss. 1997. 11: 1485- 92.
Darbar D, Gillepsie N, Choy AM, Lang CC, Pringle SD, and Pringle TH et al. Diagnosing left ventricular dysfunction after myocardial infarction: the Dundee algorithm. QJM 1997; 90: 677-83.
Poulsen SH, Jensen SE, Egstrup K. Longitudinal changes and prognostic implications of left ventricular diastolic function in first acute myocardial infarction. Am Heart J. 1999; 137: 910-8.
Coucelo J, Joaquim N. Calculation of volumes and systolic indices of heart ventricle from Halobatrachus didactylus. J Exp Zool. 2000; 286: 585 –95.
Yorchuk KJ, Davies RA, Chang KL. Measurement of left ventricular ejection fraction by acoustic quantification and comparison with radionuclide angiography. Am J Cardiol. 1994; 74: 1052-56.