Common risk factors of non-adherence antihypertensive medication and its determinants among patients
Abstract
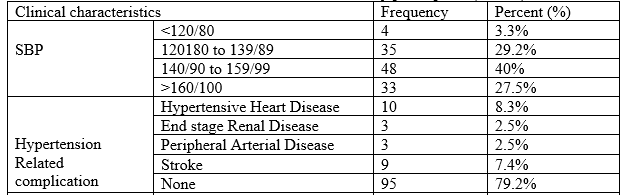
Background: Adherence to pharmacological treatment for hypertension is considered a key factor in guaranteeing successful therapy outcomes. Non-adherence to antihypertensive therapy can be determined by demographic, drug related, disease related and setting related factors. Objective: To assess the common risk factors of non-adherence antihypertensive medication and its determinants among patients. Methods: A prospective cross-sectional study was conducted at Cardiology Dept. Islami Bank Community Hospital Faridpur and 250 Bedded General Hospital, Gopalgonj, Bangladesh July to December 2021. A total of 120 patients were interviewed with a structured standard questionnaire and patient medication charts were reviewed. The questionnaire contained of demographic questions and characteristics of hypertension and its therapy. The data collected were cleaned, entered and analyzed using Statistical Package for Social Science (SPSS) version 19 for windows with 95% confidence interval and P value <0.05. Results: Total 120 study participants were interviewed of which 74 (61.7%) were female and 46 (38.3%) were males. The mean age of respondents was 54.7±12.7 years. Forty-five (37.5%) of the participants were at the age of above 60 years and 81 (67.5%) were illiterate. A large proportion of the subjects, 85 (70.8%), were married and 40 (33.3%) of the total study population were unemployed while 30 (25%) were housewives. Around one fourth (25%) of the study participants were found to be non-adherent to their treatment. Family support on adherence (AOR = 0.170, 95%CI = 0.030-0.905), spot blood pressure (AOR = 0.052, 95%, CI =0.003-0.242), place of patient residence (AOR=0.184, 95%CI =0.024-0.597) and hypertension related complications (AOR= 21.737, 95%CI =1.568-418.428) were found significantly and strongly associated with treatment non-adherence. Conclusions: In conclusion, this study were completely non-adherent and only around half of them were adherent to their medications. The absences of family support, being at the prehypertension class of blood pressure, hypertensive heart disease were shown to decrease adherence to antihypertensive medications. Therefore, health care professionals should be adequately trained and resourced to offer proper counseling to hypertensive patients on their medication and disease conditions.
Downloads
References
Rampal L, Rampal S, Azhar MZ, Rahman AR. Prevalence, awareness, treatment and control of hypertension in Malaysia: a national study of 16440 subjects. Public Health. 2008;122(1):11-8.
Rodgers A, Lawes C, MacMahon S. Reducing the global burden of blood pressure-related cardiovascular disease. J Hypertens Suppl. 2000;18(1):S3-6.
Eduardo S, Avenue A. Adherence to long term therapies evidence for action. WHO, 2003. Available at: http://www.who.int/chp/knowledge/publications/adh erence_report/en/.
Nichols-English G, Poirier S. Optimizing adherence to pharmaceutical care plans. J Am Pharm Assoc. 2000;40:475-85.
Haynes RB, McDonald H, Garg AX, Montague P. Interventions for helping patients to follow prescriptions for medications. Cochrane Database Syst Rev. 2002;(2):CD000011.
Felkey BG. Adherence screening and monitoring. Am Pharm. 1995 Jul;NS35(7):42-51.
Meichenbaum D, Turk DC. Facilitating treatment adherence. In: Meichenbaum D, Turk DC. A, eds. Practitioner’s Guidebook. New York, NY: Plenum Press; 1987: 20.
Haruna AJ. Adherence to anti-hypertensive medication regimens among patients attending the G.P.H.A. Hospital in Takoradi - Ghana, 2006. Available at: http://ir.knust.edu.gh/bitstream/123456789/677/1/H ARUNA%20AHMED%20JAMBEDU.pdf.
Fatmah A, Xiang-Yu H, Ignacio C. Factors affecting antihypertensive treatment adherence: a Saudi Arabian perspective. Clin Med Diagn. 2012;2(4):27- 32.
Hayden B. Bosworth. Medication adherence: making the case for increased awareness, 2012. Available at:
Ambaw AD, Alemie GA, W/Yohannes SM, Mengesha ZB. Adherence to antihypertensive treatment and associated factors among patients on follow up at University of Gondar hospital, Northwest Ethiopia. BMC Public Health. 2012;12:282.
Hashmi SK, Afridi MB, Abbas K, Sajwani RA, Saleheen D, Frossard PM, et al. factors associated with adherence to anti-hypertensive treatment in Pakistan. PLoS One. 2007;2(3):e280.
Brigitte R Martins dos S, Juliana T, Débora G, Reynaldo MG, Boni Y, Cicera CVA. Blood pressure levels and adherence to treatment of hypertensive patients, users of a school pharmacy. Braz J Pharm Sci. 2010;46(3):421-30.
Timothy JC. Adherence to hypertension management recommendations for patient follow-up care and lifestyle modifications made by military healthcare providers, May 2000. Available at: http://www.dtic.mil/get-trdoc/pdf?AD=ADA421146.
J. M. Flack, S. V. Novikov, C. M. Ferrario. Benefits of adherence to anti-hypertensive drug therapy. Eur Heart J.1996;17(Suppl A):16-20.