To Identify the Clinical Parameters Suggestive of Stroke in Patients Presenting to Emergency Department with Vertigo
Abstract
Background and Purpose: Investigating every vertigo patient for central or peripheral MRI and other treatments is expensive and taxing for the system. Thus, emergency physicians must identify stroke patients and give immediate treatment to minimize disastrous results.
Methods: 500-bed BGS Global hospital prospective cohort research. Consecutive vertigo patients endure history, head impulse, nystagmus, skew deviation, and neurological symptoms such leg or truncal ataxia. Scheduled brain MRIs. MRI found strokes. Clinical assessment and normal MRI found peripheral lesions.
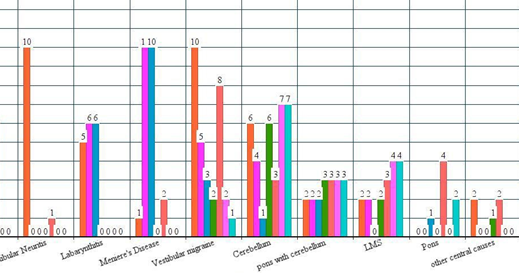
Results: Of the 102 acute vertigo patients, 70 were peripheral and 32 central (29 posterior circulation stroke, 2 anterior circulation, and 1 central venous thrombosis). Vertigo patients averaged 49.64706 ± 14.3931 (SD). 36 women, 66 males (64.3%). ED presentation averages 12.54902 ± 10.76355 (SD) hours. Central and peripheral causes were explored. Vomiting, hearing problems, headaches, and tinnitus did not discriminate central from peripheral causes (p <0.01). Diplopia, Dysphagia, Dysarthria, Head impulse test, Nystagmus examination, Skew deviation test, and neurological indicators such limb or truncal ataxia separate central from peripheral causes (p <0.01). Diplopia, Dysarthria, Dysphagia, Nystagmus, Skew deviation, and ataxia have poor sensitivity and high specificity. High-sensitivity, low-specificity head impulse test. This study shows that individual characteristics cannot distinguish central from peripheral vertigo. The study showed good sensitivity 92.31% (0.63 to 0.99) and specificity 100% (0.87 to 1). This test distinguishes central from peripheral vertigo.
Conclusions: Absence of Diplopia, Dysphagia, Dysarthria, abnormal head impulse test, No direction-changing Nystagmus, and absence of Skew deviation in the first clinical visit with vertigo can reliably exclude central cause and discharged home from ED safely without further investigations and imaging.
Downloads
References
Flomann E, Rothwell PM. Prognosis of vertebrobasilar transient ischaemic attack and minor stroke. Brain. 2003;126:1940-1954.
Louis R Caplan M. Up To Date: Etiology, classification, and epidemiology of stroke. Available at: http://www.uptodate.com/contents/etiology- classification-andepidemiology of- stroke? Accessed 03/23, 2015.
Mantokoudis G, Saber Tehrani AS, Wozniak A, et al. VOR Gain by Head Impulse video-Oculography Differentiates Acute Vestibular Neuritis from Stroke. Otol Neurotol.2015;36:457-465
Savitz SI, Caplan LR. Vertebrobasilar disease. N Engl J Med. 2005;352:2618-2626.
Lee H, Sohn SI, Cho YW, et al. Cerebellar infarction presenting isolated vertigo: Frequency and vascular topographical patterns. Neurology. 2006;67:1178-1183.
Saber Tehrani AS, Coughlan DMP, Hsieh YH, et al. Rising Annual Costs of Dizziness Presentations to U.S. Emergency Departments. Acad Emerg Med. 2013;20:689-696.
Tarnutzer AA, Berkowitz AL, Robinson KA, Hsieh Y, NewmanToker DE. Does my dizzy patient have a stroke? A systematic review of bedside diagnosis in acute vestibular syndrome. CMAJ Canadian Medical Association Journal. 2011;183:E571-E592.
James A. Nelson, MD*.Erik Viirre MD, “PhD The Clinical Differentiation of Cerebellar Infarction from Common Vertigo Syndromes.”
David E. Newman-Toker, Ernest Moy, Ernest Valente, Rosann Coffey and Anika L. Hynes. Missed diagnosis of stroke in the emergency department: a cross-sectional analysis of a large population based sample. Diagnosis 2014 dx 2013-0038.
Kattah JC, Talkad AV, Wang DZ, Hsieh YH, Newman-Toker DE. HINTS to diagnose stroke in the acute vestibular syndrome: Three-step bedside oculomotor examination more sensitive than early MRI diffusion-weighted imaging. Stroke. 2009; 40 (11): 3504-3510
Kothari R, Hall K, Brott T, Broderick J. Early stroke recognition: Developing an out-of –hospital NIH Stroke Scale. Acad Emerg Med. 1997; 4: 986-990
D. Eric Searls, MD; Louis R. Caplan, MD et all “ Symptoms and Signs of Posterior Circulation Ischemia in the New England Medical Center Posterior Circulation Registry.”
Amre Nouh, Jessica Remke et al in Ischemic Posterior Circulation Stroke: A Review of Anatomy, Clinical Presentations, Diagnosis, and Current Management
James Wright, MD; Christina Huang, MD; Daniel Strbian, MD, PhD; Sophia Sundararajan, MD, PhD et al Diagnosis and Management of Acute Cerebellar Infarction shows.