Use of the Robson classification to assess, normal delivery and caesarean section trends in a Tertiary Care Hospital
Abstract
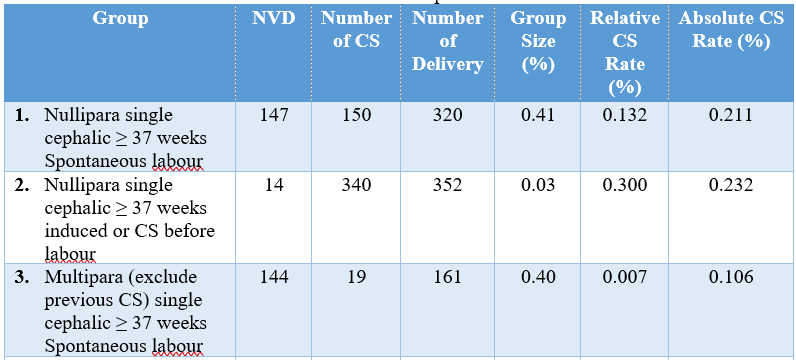
Background: Robson ten-group classification system is recommended by WHO (World health organization) as a global standard for assessment and monitoring caesarean section (CS) rates. This classification is simple and robust. It is prospective, easily reproducible and clinically relevant. The Robson classification, or Ten Group Classification System (TGCS), is a widely recognized framework for evaluating caesarean section rates and delivery trends in maternity care settings. By categorizing women into ten distinct groups based on key obstetric characteristics, the classification allows for a standardized and systematic approach to monitoring and comparing delivery practices. Objectives: The aim of the study was to evaluate the use of the Robson classification to assess, normal delivery and caesarean section trends in a tertiary care hospital. Methods: This cross-sectional observational study was conducted over one year at OGSB Hospital and Institute of Reproductive & Child Health, Dhaka, Bangladesh during January 2023 to December 2023. All pregnant women admitted for delivery at ≥28 weeks of gestation were included and categorized into ten groups according to the TGCS based on specific obstetric characteristics. Data were collected using a structured questionnaire and extracted from medical records. Descriptive statistics were used to analyze the distribution of women across the Robson groups, group-specific CS rates, and the contribution of each group to the overall CS rate. Statistical analyses of the results were be obtained by using window-based Microsoft Excel and Statistical Packages for Social Sciences (SPSS-24). Results: The group of Nullipara single cephalic ≥ 37 weeks spontaneous labor (Group 1) had 150 CS and 320 deliveries. The group size, CS rate, and absolute group contribution to overall CS were 0.41%, 0.132%, and 0.211%, respectively. Another notable category includes nulliparous women with single cephalic pregnancies at 37 weeks or more who had induced labor or a CS before labor (category 2), which accounted for 0.03% of deliveries, had a high CS rate of 0.30%, and contributed 0.23% to the total rate. Conclusion: The utility of the Robson classification in identifying areas where caesarean sections may be overused, particularly in low-risk groups, and in evaluating the effectiveness of clinical interventions aimed at promoting normal deliveries. The regular use of the Robson classification in clinical practice can provide valuable insights into delivery trends, support evidence-based decision-making, and contribute to improved maternal and neonatal outcomes in tertiary care settings.
Downloads
References
Unicef. The State of the World’s Children 2013. New York: UNICEF, 2013.
Maine D. Monitoring emergency obstetric care: a handbook. World Health Organization; 2009.
Althabe F, Belizán JM. Caesarean section: the paradox. The Lancet. 2006 Oct 28;368(9546):1472-3.
Robson MS. Classification of caesarean sections. Fetal and maternal medicine review. 2001 Feb;12(1):23-39.
Betrán AP, Torloni MR, Zhang JJ, Gülmezoglu AM, Aleem HA, Althabe F, Bergholt T, De Bernis L, Carroli G, Deneux‐Tharaux C, Devlieger R. WHO statement on caesarean section rates. Bjog. 2016 Apr;123(5):667.
Mahadik K. Rising cesarean rates: are primary sections overused? The Journal of Obstetrics and Gynecology of India. 2019 Dec;69(6):483-9.
Abdel-Aleem H, Shaaban OM, Hassanin AI, Ibraheem AA. Analysis of cesarean delivery at Assiut university hospital using the ten-group classification system. International Journal of Gynecology & Obstetrics. 2013 Nov 1;123(2):119-23.
Betrán AP, Torloni MR, Zhang JJ, Gülmezoglu AM, Aleem HA, Althabe F, Bergholt T, De Bernis L, Carroli G, Deneux‐Tharaux C, Devlieger R. WHO statement on caesarean section rates. Bjog. 2016 Apr;123(5):667.
Sandall J, Tribe RM, Avery L, Mola G, Visser GH, Homer CS, Gibbons D, Kelly NM, Kennedy HP, Kidanto H, Taylor P. Short-term and long-term effects of caesarean section on the health of women and children. The Lancet. 2018 Oct 13;392(10155):1349-57.
Betran AP, Torloni MR, Zhang J, Ye J, Mikolajczyk R, Deneux-Tharaux C, Oladapo OT, Souza JP, Tunçalp Ö, Vogel JP, Gülmezoglu AM. What is the optimal rate of caesarean section at population level? A systematic review of ecologic studies. Reproductive health. 2015 Dec; 12:1-0.
Loue VA, Gbary EA, Koffi SV, Koffi AK, Traore M, Konan JK, N’Drin D, Abauleth RY, Kouakou F, Boni SE. Analysis of caesarean rate and indications of university hospitals in sub-Saharan African developing countries using Robson classification system: the case of Cocody’s hospital center, Abidjan-Cote d’Ivoire. Int J Reprod Contracept Obstet Gynecol. 2016 Jun 1;5(6):1773-7.
Kelly S, Sprague A, Fell DB, Murphy P, Aelicks N, Guo Y, Fahey J, Lauzon L, Scott H, Lee L, Kinniburgh B. Examining caesarean section rates in Canada using the Robson classification system. Journal of Obstetrics and Gynaecology Canada. 2013 Mar 1;35(3):206-14.
Robson SJ, De Costa CM. Thirty years of the World Health Organization's target caesarean section rate: time to move on. Medical journal of Australia. 2017 Mar;206(4):181-5.
World Health Organization. Robson classification: implementation manual.
Kelly S, Sprague A, Fell DB, Murphy P, Aelicks N, Guo Y, Fahey J, Lauzon L, Scott H, Lee L, Kinniburgh B. Examining caesarean section rates in Canada using the Robson classification system. Journal of Obstetrics and Gynaecology Canada. 2013 Mar 1;35(3):206-14.
Delbaere I, Cammu H, Martens E, Tency I, Martens G, Temmerman M. Limiting the caesarean section rate in low-risk pregnancies is key to lowering the trend of increased abdominal deliveries: an observational study. BMC pregnancy and childbirth. 2012 Dec; 12:1-0.
Robson M. The Ten Group Classification System (TGCS)-a common starting point for more detailed analysis. BJOG: An International Journal of Obstetrics & Gynaecology. 2015 Apr 1;122(5).