Study of clinical profile and management of age-related macular degeneration at rural tertiary care hospital
Abstract
Introduction: Age-related macular degeneration (ARMD) is the leading cause of irreversible blindness in elderly population after 5th decade. It is a degenerative disorder affecting macula, characterized by drusens and RPE changes. Choroidal neovascularization (CNV) and Pigment epithelial detachment (PED). Age, Gender, Smoking, Hypertension, Diabetes mellitus, Atherosclerosis, Obesity, Family history, Dietary habits are its known associated risk factors.
Aims/Objective: To Study Clinical profile, Risk factors and Management protocols in patients of Age Related Macular Degeneration at Rural Tertiary Care Hospital
Material and Methods: An observational, descriptive cross-sectional Hospital based study was conducted at a tertiary care hospital. Total 50 patients were evaluated through structured proforma. Patient’s personal history, medical history, family history, alcohol consumption, smoking, systemic illness history like Diabetes mellitus, hypertension, were studied. Dilated Fundoscopic Examination readings was taken from OPD Patient records. Direct ophthalmoscopy and Slit lamp biomicroscopy with 90D lens were conducted. Management protocols were noted like Medical management, optical management, Reference to higher center. All patients of ARMD Attending Rural Tertiary Care hospital and Patients willing to participate in the study were included. Patients below 40 years of age and Patient having optical media opacities, Myopia, Uveitis, Glaucoma, Cataract, Vitreo retinal diseases were excluded.
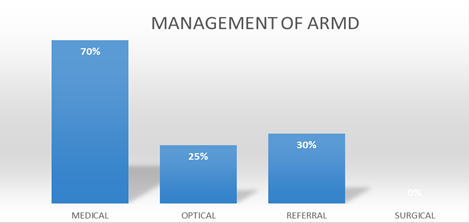
Results: Out of 50 study patients, 60% were Females. Most common age group observed was 61-70 years of age. Dry ARMD was seen in 70% patients, Wet ARMD was seen in 30 % patients. Visual acuity was more affected in Wet ARMD than Dry ARMD. Most common risk factors associated with ARMD were history of Hypertension in 70% patients, followed by Diabetes in 55%, Smoking in 57%, Alcohol consumption in 52% patients. Medical treatment was advised to 70% patients; Optical aids were given to 25% patients. 30% patients were referred to higher center; no surgical management was offered to any patients.
Conclusion: ARMD is more commonly seen in patients above 60 years of age and more in females. Dry ARMD seems to be more common than Wet ARMD, however visual disability is more in Wet ARMD.
Downloads
References
Białek-Szyma´nska A, Misiuk-Hojło M, Witkowska K. Risk factors evaluation in age related macular degeneration. Klin Oczna. 2007; 109:127–30.
World Health Organization. Age Related Macular Degeneration: Disease control and prevention of visual impairment in global initiative for the elimination of Avoidable Blindness Action Plan 2006–2011.
Kanski J, Bowling B (2016) Kanski clinical ophthalmology. 8th edition, China, Elsevier 928. Link: https://tinyurl.com/y5m544xy
Klaver CC, Assink JJ, Leeuwen RV, Wolfs RC. Incidence and progression rates of age related maculopathy, the Rother Dam Study. Invest Ophthalmol Vis Sci. 2001; 42:2237–41.
Klein BE, Klein R, Lee LE. Measures of obesity and age-related eye diseases. Ophthalmic Epidemiol. 2001; 8:251–6
Pokhrel S, Malla OK, Pradhananga CL, Joshi SN. A Pattern of
Age-related Macular Degeneration. JNMA J Nepal Med Assoc.
;48(175):217–20.
Tan JS, Mitchell P, Kifley A, Flood V, Smith W, Wang JJ. Smoking
and the longterm incidence of age-related macular degeneration: The
Blue Mountains Eye Study. Arch Ophthalmol. 2007; 125:1089–95.
Singare RP, Deshmukh S, Ughade SN, Thakre SB. Agerelated macular degeneration: Prevalence and risk factors in elderly population (aged >60 years) in India. Int J Sci Res Pub. 2015;5(2):1–6.
Monocyte activation in patients with age-related macular degeneration: a biomarker of risk for choroidal neovascularization. Arch Ophthalmol. 2004; 122(7):1013–8.
Hyman L, Schachat AP, He Q, et al.: Hypertension, Cardiovascular Disease, and Age-related Macular Degeneration. Arch Ophthal 2000, 117:351–358
Seddon JM et al.: A Prospective Study of cigarette smoking and Age-Related
Macular Degeneration in women. JAMA 1996, 276:1141–1146.
Nirmalan PK. Prevalence of Vitreoretinal Disorders in a Rural
Population of Southern India. Arch Ophthalmol. 2004;122(4):581–6.
Ritter, LL, Klein, R, Klein, BE, et al; Alcohol intake and age related maculopathy in the
Beaver Dam Eye Study, Am J Ophthalmol 120:190-196, 1995
Smith, W, and Mitchell, P: Alcohol intake and age related maculopathy, Am J Ophthalmol 122:743-745, 1996
Choi JK, Lym YL, Moon JW, Shin HJ, Cho B (2011) Diabetes mellitus and early age-related macular degeneration. Arch Ophthalmol 129: 196–199.
Chen X, Rong SS, Xu Q, Tang FY, Liu Y, Gu H, et al. (2014) Diabetes Mellitus and Risk of Age-Related Macular Degeneration: A Systematic Review and Meta-Analysis. PLoS ONE 9(9): e108196. https://doi.org/10.1371/journal.pone.0108196
Wamg, JJ, Mitchell, P, and Smith, W: Refractive error and age related maculopathy: The Blue Mountains Eye Study, Invest Ophthalmol Vis Sci 39:2167-2171,1998
Jayashree MP, Harika JV, Arathi C, Patil BA, Niveditha RK. Prevalence of age related macular degeneration in a tertiary care centre. Journal of Clinical Research and Ophthalmology. 2019 May 23;6(1):007-10.
Age-Related Eye Disease Study Research Group. SanGiovanni JP, Chew EY, Clemons TE, Ferris FL, Gensler G, Lindblad AS, Milton RC, Seddon JM, Sperduto RD. The relationship of dietary carotenoid and vitamin A, E, and C intake with age-related macular degeneration in a case-control study: AREDS Report No. 22. Arch Ophthalmol. 2007 Sep;125(9):1225-32.
Gopalakrishnan S, Velu S, Raman R. Low-vision intervention in individuals with age-related macular degeneration. Indian Journal of Ophthalmology. 2020 May;68(5):886.